Brantova O.I., Tweneboa Kodua Kwaku
Kyiv, Ukraine
Introduction
Dizziness is experienced by more than 20% of Global population. It is the 3rd most common reason for patient admittance to the doctor in the USA. According to a Cochrane review, based on a screening of a national representative sample of 4869 adults living in Germany, Dizziness/Vertigo has a prevalence of 22.9% and an incidence of 3.1%.
Only 1.8% of the unselected adults consulted a physician in the last 12 months for dizziness/vertigo (0.9% for vertigo). Also 28.5% complained about poor tolerance to high places, or simply the fear of height(acrophobia), which is also related to vestibular disorders. Low sensitivity, lack of exact topic diagnostics, low tolerability, limited utility for management and high price of modern Vertigo Laboratory equipment has resulted in the restriction of its routine use.
Therefore, 20-point Test Battery has been proposed. The normative data for it has been ruled out in 80-th and only for Kyiv citizens. The aim of the current study is to evaluate the coordination function of students from European (Ukrainians), Asian (mostly Indian) and African continents.
Materials and methods
91 students have been examined with the mean age of 20,25±3,99 years, among them are 53 males and 38 females with an average height of 171,98±9,33 cm and weight of 66,81±13,53 kg. None of them has ever complained of vertigo or dizziness. Among the examined students, 43 people are Ukrainian (m – 16, f – 27), 13 – African (m – 9, f – 4), and 45 Asian (m – 28, f – 7) students. All the students volunteered to take part in the examination, free of charge.
20-point test battery for express-diagnostics of coordination function [4]
Complaints quantification
Dizziness attacks are considered to be significant when their duration is more than one minute and frequency is more than once per month. It is also taken into consideration additional symptoms: headache, black-outs, nightmares, tinnitus, memory problems, depressions and consciousness losses related to dizziness attacks. [1; 8].
Standardized results are described as following:
- 0 points – complaints are absent;
- 1 point – complaints of dizziness (or vertigo) which duration exceeds 1 minute;
- 1 – complaints of dizziness which frequency exceeds once per month;
- 1 point – complaints of accompanying symptoms.
Possible signs combination might be expressed in figures from 0 to 3.
Uemura test
Standing on one foot with eyes closed. If the patient is stable at one foot with eyes closed more than 10s he is considered to be healthy.
Uemura test is evaluated in 5 point score:
- 0 points – patient is stable for 10s with eyes closed at one foot;
- 1 – undulating moderately, but keeping balance;
- 2 – hands are needed to keep balance (hand is reaching shoulder level);
- 3 – cannot stand at a spot or stands 3-10 s;
- 4 – cannot stand at one foot even 3 s;
- 5 – cannot stand even at two feet.
Lateralization of displacements and falls are sometimes important.
Stepping (walking) fukuda test
Three principal parameters are considered during this test:
- displacement distance;
- displacement angle;
- spin (rotation) angle [2].
Normal is forward linear displacement at the distance of 0.2-1.0 m, angle up to 300 and rotation up to 300.
Test evaluation is proceeded with three score system:
- 0 – points forward displacement at distance of 0.2-1.0 m, displacement and spin to the angle up to 300;
- 1 – displacement less than 0.2 m or more than 1.0 m;
- 1 – displacement at the angle more than 300;
- 1 – spinning at the angle more than 300.
Backward displacement is considered to be extremely bad, because it reveals the distortion of space orientation and must be evaluated as 3 points.
Fukuda writing test
Patient is asked to write “33” in column with eyes closed [8]. For healthy individuals it is easy going.
Standardization of the results looks as following:
- 0 – column is straight;
- 1 – column is undulating;
- 2 – column decline more than 300;
- 3 points – dismetria.
Tracking
The patient is asked to track a small bright subject, moving horizontally and vertically. Subject is placed at the eyes level.
Quantification of test results is the following:
- 0 – tracking is smooth in all the eyes positions;
- 1 – non-smooth in lateral positions;
- 2 – non-smooth not only in lateral positions;
- 3 points – spontaneous eye movements (nystagmus, saccades).
Indicating (past pointing test)
The patient is asked to point with a pen or pencil the target with eyes closed at the distance of stretched hand. Results might be fixed at the sheet of paper, monitor screen, etc.
Quantification means:
- 0 point – point in the diameter of 25 mm;
- 1 – pointing diameter 50 mm;
- 2 – pointing diameter 75 mm;
- 3 – pointing outside diameter 75 mm.
Direction of mispointing is fixed separately.
According to the result of all the tests vestibular function is evaluated from 0 to 20 points. Figures from 0 to 4 are characterizing norm, 5-9 points indicate small degree of vestibular dysfunction, 10-14 – moderate pathology, and 15-20 – severe lesion. The sensitivity of such test battery reaches 93.64% (n=912) [5].
Results
The general results are presented in the Table 1.
| Table 1.General results for all the students | |||
| № | Parameter studied | Mean | Standard deviation |
| 1 | Height cm | 171.98 | 9.33 |
| 2 | Weight kg | 66.81 | 13.53 |
| 3 | Uemura | 0.88 | 0.89 |
| 4 | Fukuda stepping | 1.01 | 0.92 |
| 5 | Fukuda writing | 0.87 | 0.83 |
| 6 | Past pointing (indicating) | 0,14 | 0.35 |
| 7 | Tracking | 0,01 | 0.10 |
| 8 | Total | 2.85 | 1.90 |
| 9 | Systolic blood pressure mm hg | 115.96 | 10.84 |
| 10 | Diastolic blood pressure mm hg | 75.54 | 8.39 |
| 11 | Pulse b/min | 80.66 | 9.39 |
As one can see we have rather typical data about height, weight, circulation function in all of the students examined.
Then we compared the parameters mentioned in Ukrainian students with all the group of foreign students. The data is presented in the Table 2.
| Table 2. Comparison of the parameters studied in Ukrainian students and in all the group of foreign students | |||||||
| № | Parameter studied | Mean Ukrain. | Mean foreign | Sigma Ukrain. | Sigma foreign | T-test | F-test |
| 1 | Height | 172.14 | 171.83 | 9.58 | 9.20 | 0.87713 | 0.782876 |
| 2 | Weight | 67.23 | 66.44 | 14.17 | 13.08 | 0.782333 | 0.591215 |
| 3 | Uemura | 0.58 | 1.15 | 0.79 | 0.90 | 0.002022 | 0.415027 |
| 4 | Fukuda stepping | 0.88 | 1.13 | 0.82 | 1.00 | 0.211055 | 0.194807 |
| 5 | Fukuda writing | 0.86 | 0.86 | 0.91 | 0.76 | 0.93498 | 0.221293 |
| 6 | Past pointing (indicating) | 0.07 | 0.21 | 0.26 | 0.41 | 0.05479 | 0.002724 |
| 7 | Tracking | 0 | 0.02 | 0 | 0.14 | 0.322431 | delet/0 |
| 8 | Total | 2.40 | 3.25 | 2.05 | 1.67 | 0.033237 | 0.1733 |
| 9 | Systolic blood pressure | 118.14 | 114.00 | 12.80 | 9.30 | 0.073106 | 0.082214 |
| 10 | Diastolic blood pressure | 76.6 | 74.59 | 8.73 | 8.03 | 0.255585 | 0.575588 |
| 11 | Pulse | 83.65 | 77.98 | 9.21 | 8.81 | 0.003593 | 0.764133 |
The result are actually wonderful!
It is obvious that the two groups are well matched in height and weight. They do not have significant difference in blood pressure (especially diastolic), but they differ in pulse rate. The difference is significant only according to T-test, which means that the difference is only quantitative and not qualitative. This difference might be because there are more tobacco smokers among the Ukrainian students. Non-significant difference in systolic blood pressure might also be caused by tobacco influence.
From the other side, one can see that coordination is better in Ukrainian students: 2.40±2.05 versus 3.25±1.67 points. It is only quantitative (T-test=0.033237, F-test=0.1733).
The most significant difference is seen in performance of past pointing test, which is mostly qualitative (F-test=0.002724, T-test=0.05479), indicating that better targetting in European students is related to some health problems, whiles in foreign students, might be problems of stress, change in geographical location or winter period.
Also interesting is the fact that Uemura test data differ significantly (0.58±0.79 and 1.15±0.90, T-test=0.002022 and F-test=0.415027), thus indicating that European students are qualitatively better at performing Uemura test.
Special interest begs the question, what is the exact difference between the different groups of students – European, African and Asian? The total score is shown at Fig. 1.
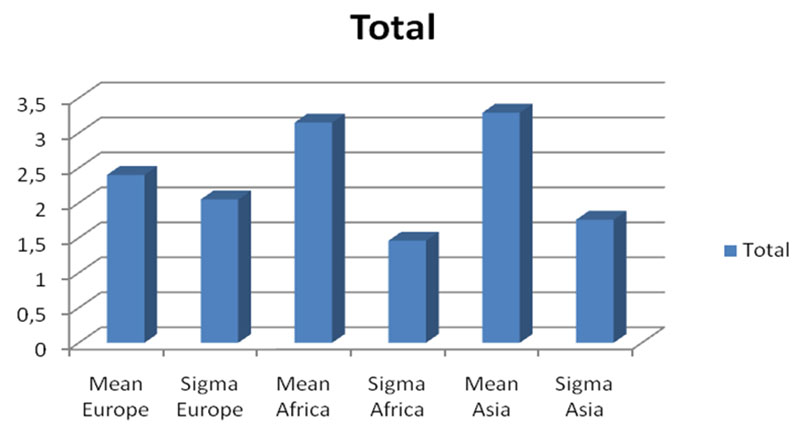
Especially interesting is the fact that students originating from African and Asian continents have worse coordination test performance than the European students. Particular interest is related to the significance of the differences from the point of view of high level of sigma for Europeans. This data is presented in Table 3.
| Table 3. Comparison of the Total score for coordiation of the students coming from different continents | ||||||
| Parameter studied | Mean Europe | Mean Africa | Sigma Europe | Sigma Africa | T-test | F-test |
| Total | 2.40 | 3.15 | 2.05 | 1.46 | 0.149909 | 0.207417 |
| Parameter studied | Mean Europe | Mean Asia | Sigma Europe | Sigma Asia | T-test | F-test |
| Total | 2.40 | 3.29 | 2.05 | 1.76 | 0.042374 | 0.361841 |
As we can see, the difference between European and Asian students is significant according to quantitative T-test, which means that it is not related to some health conditions, but it is just specific to the Asian people.
The differenc in coordination performance of the African and Asian students appeared to be negligible. It has been interesting to find out if there are differences between the separate tests. This data are presented in the Tables 4 and 5.
| Table 4. Comparizon of the coordination test performance by European and African students | ||||||
| Parameter studied | Mean Europe | Mean Asia | Sigma Europe | Sigma Asia | T-test | F-test |
| Uemura | 0.58 | 1.20 | 0.79 | 0.93 | 0.002539 | 0.317683 |
| Fukuda stepping | 0.88 | 1.11 | 0.82 | 1.02 | 0.284294 | 0.179932 |
| Fukuda writing | 0.86 | 0.80 | 0.91 | 0.76 | 0.740257 | 0.265191 |
| Past pointing (indicating) | 0.07 | 0.29 | 0.26 | 0.46 | 0.017565 | 0.000477 |
| Tracking | 0 | 0.03 | 0 | 0.17 | 0.000784 | delet/0 |
| Table 5. Comparison of the coordination test performance by European and Asian students | ||||||
| Parameter studied | Mean Europe | Mean Africa | Sigma Europe | Sigma Africa | T-test | F-test |
| Uemura | 0.58 | 1.00 | 0.79 | 0.78 | 0.120229 | 0.835724 |
| Fukuda stepping | 0.88 | 1.15 | 0.82 | 0.99 | 0.381996 | 0.37303 |
| Fukuda writing | 0.86 | 1.08 | 0.91 | 0.76 | 0.40028 | 0.49554 |
| Past pointing (indicating) | 0.07 | 0 | 0.26 | 0 | 0.083175 | delet/0 |
| Tracking | 0 | 0 | 0 | 0 | delet/0 | delet/0 |
As it is shown at the Table 4 there is no difference in the separate test performance between European and African students. There is also no significant difference between coordination of African and Asian students.
But there is significant difference between European and Asian students, especially in performing of the past pointing and tracking test.
Thus, concidering the whole bulk of the data we see, there is significant difference in the coordination performance between European and foreign, especially Asian continent students. This data corresponds to the previous literary data 2.13±1.31 points being the normative value. According to previous calculations it has been proposed to consider 5-6 point to be the borderline for health and pathology [6]. That means that coordination performance is normal in all the student groups studied.
Discussion
20-point test battery for express-diagnostics of coordination function has appeared to be useful to study occupational pathology in tractor drivers [7], miners [3], Chornobyl clean-uppers [6].
Our present study shows that there is the difference in the coordinatiion test performance of the young people originating from different continents. This phenomenon yet has no explanation and needs future investigation. This difference must be taken into concideration while preparing standards for different contingents.
Conclusion
Young people (students) from different continents have different performance of coordination tests: the best performance was exhibited by the European students, then comes African and finally followed by students from Asia.
Literature
- Claussen C.F. Schwindel, symptomatik, diagnostik, therapie. – Hamburg, Edition m+p. Dr. Werner Rudat und Co, 1983. – 225 p.
- Fukuda T. The stepping test: 2 phases of the labyrinthine reflex. Acta Otolaryng (Stockh.). 1959, 50, 95-108.
- Nikolenko VYu. Diseases of nervous system in miners and immune pathology (in Ukrainian). Donetsk. 1999, 266 P.
- Trinus K.F. Chornobyl vertigo. 10 years of monitoring. Neurootology Newsletter, 1996, Suppl. 1, 140 p.
- Trinus K.F. Dizziness study test comparizon. Archives of sensology and neurootology in science and practice ASN, 2011, Vol. 6. ISSN 1612 3352 http://neurootology.org
- Trinus K. Vestibular system: morpho-physiology and pathology. Lambert Academic Publishing. 2012, 544 p. ISBN 978-3-659-11350-5
- Trinus K.F., Oleinik V.I., Cherniuk V.I., Lastovchenko V.B., Meshcheriakov G.V., Nikolenko V.Y. Vestibular traumatic action of the different loadings. Vertigo, nausea, tinnitus and hypoacusia due to head and neck trauma. Claussen C.-F., Kirtane M.V. eds., Elsevier Science Publishers, 1991, 171-174.
- Uemura T., Suzuki J.-I., Hozawa J., Highstein S.M. Neurootological examination with special reference to equilibrium function tests. Tokyo, Igaku Shoin Ltd., 1977, 178 p.